Інші зображення цього випадку

Image
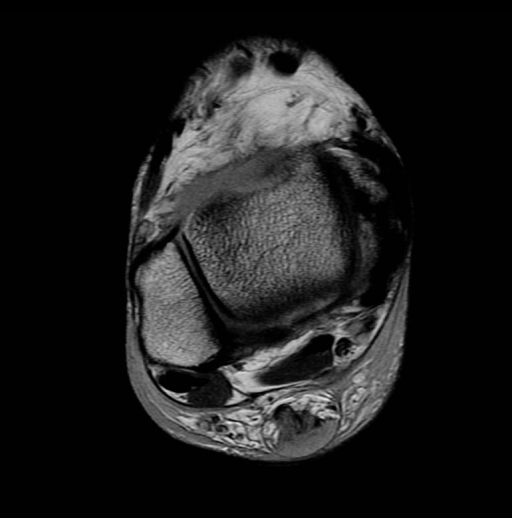
Achilles tendon tear
- Image ID
- MPX2485_synpic24205
- Case U_id
- MPX2485
- Modality
- MR · MR - T1W - noncontrast
- Plane
- Axial
- Location
- Musculoskeletal (Spine and Muscles)
- Age / Sex
- 70 / male
- Caption
- MRI Images
- ACR Codes
- 4.4
Clinical case
- History
- 70 y/o male who felt a “pop” two days prior to presentation and has had pain in region of right Achilles tendon since that time.
- Exam
- Tenderness to palpation in posterior aspect of right ankle
- Findings
- MRI: Proton density without fat sat axial shows medium signal intensity in the region of the Achilles tendon and fat obliteration This medium signal intensity becomes high signal intensity on T2 weighted with fat sat, with extensive edema medial, lateral, and posterior to the tendon T1 weighted sagittal reveals complete disruption approximately 5cm above the insertion site into the calcaneus. This disruption approximately 4cm proximally. Sonography: longitudinal image on sonogram in region of Achilles tendon demonstrating heterogeneous echotexture with posttraumatic inflammation and hemorrhage.
- Differential Diagnosis
- Complete Achilles tendon tear
- Case Diagnosis
- Achilles tendon tear
Topic
- Category
- Trauma
- ACR Code
- 4.4
Disease discussion
): The Achilles tendon is the largest tendon in the body and is formed by the confluence of the gastrocnemius and soleus muscle complexes. The tendon is vulnerable to complete and partial tears. Trauma is involved In the majority of cases of Achilles tendon injury. However, there are many conditions that may weaken the tendon and predispose it to injury. These include degenerative changes, tissue ischemia, floroquinalone use, and systemic diseases such as rheumatoid arthritis, systemic lupus erythematosus, diabetes mellitus, and gout. The stereotypical patient is a middle-aged individual who is out of condition and starts playing a sport. The mechanism of injury is commonly forced dorsiflexion and the patient often reports an audible “pop”. Symptoms include pain, swelling, and weakness of plantar flexion, but often tears are asymptomatic.
Diagnosis of an Achilles tendon rupture is often made by history and physical examination alone. However, up to 25% of cases can be missed without imaging. Physical exam findings include tenderness in the region of the tendon, positive Thompson test (absent plantar flexion on squeezing of the calf), or a palpable focal cleft at the insertion of the tendon. Imaging diagnosis is made with either MRI or sonography. With MRI, an intact tendon should have low signal intensity in all sequences. Increased intensity in any sequence is consistent with a tear in the tendon or tendonitis. Partial or complete disruption of the fibers is diagnostic for a tear in the tendon. With sonography the intact tendon has homogeneous low-level echoes oriented lengthwise along the tendon. Complete tears are characterized by discontinuity of the tendon, often with fluid in the gap and variable irregular echogenicity of Kaeger’s fat pad due to hemorrhage and edema. Ultrasound has been shown to be highly reliable in diagnosing complete tendon rupture, as well as differentiating full from partial-thickness tears. Ultrasound can be used for diagnosis of both partial and complete tear of the tendon.
Treatment is controversial and is largely based on the individual patient. Patients who are older, less active, or who are poor surgical candidates are generally treated with serial casting. This non-surgical approach is associated with re-rupture (particularly in the first four weeks after the cast has been removed) and venous thrombosis. Surgical repair is suited for young, active patients; however, the incidence of complications with surgical repair is reported to be 20%.