Image
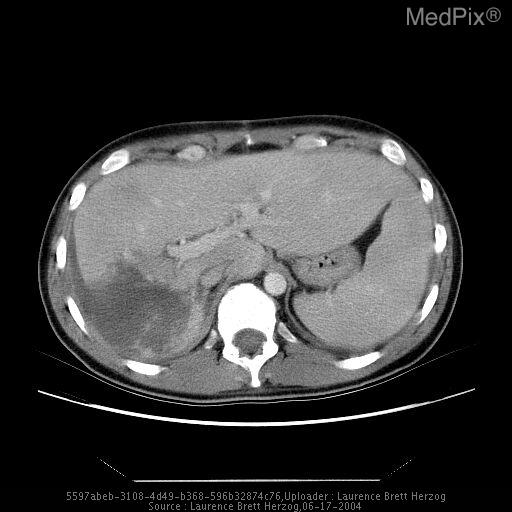
Hepatic laceration with biloma.
- Image ID
- MPX2423_synpic20203
- Case U_id
- MPX2423
- Modality
- CT · CT - GI & IV Contrast
- Plane
- Axial
- Location
- Gastrointestinal (Abdomen)
- Age / Sex
- 29 / male
- Caption
- Helical axial CT with or and IV contrast demonstrates an irregular defect within the right lobe of the liver extending peripherally consistent with a post-traumatic liver laceration. Associated fluid density is seen without extravasation of neither intravenous contrast material nor large space occupying lesion compression the right lobe. A hematoma versus biloma was on the differential.
- ACR Codes
- 7.4
Clinical case
- History
- 29 y/o male s/p liver laceration with repair three weeks ago.
- Findings
- Findings include a fluid density on CT within the right upper quadrant adjacent to the liver. Loculations and septations may be present as well. An adjacent hepatic parenchymal defect is often present. As they mature, bilomas usually appear round with a thin surrounding capsule. Free intra-peritoneal fluid collections can indicate biloma rupture. Only biliary scintigraphy, can definitively demonstrate a communication between the biliary tree and the biloma contents.
- Differential Diagnosis
- Biloma, hematoma, seroma, abscess
- Case Diagnosis
- Hepatic laceration with biloma.
- Diagnosis By
- Biliary scintigraphy.
Topic
- Category
- Trauma
- ACR Code
- 7.-1
Disease discussion
Hepatic injuries occur in roughly 5-10% of patients with blunt abdominal trauma; other associated visceral injuries are very common. Capsular disruption and intraperitoneal hemorrhage is often present. The mortality, which is relatively high (10-25%), is usually due to either an associated injury or an uncontrollable hemorrhage from a laceration or a central burst that involves the major hepatic veins and/or the intrahepatic or retrohepatic inferior vena cava. These latter patients rarely come to CT because of instability. Contrast-enhanced CT is the procedure of choice for evaluating hepatic injuries in stable patients. It can define the extent of injury, detect associated injuries and roughly quantitate the amount of hemoperitoneum. The amount of hemoperitoneum does not always correlate with clinical stability and the need for immediate surgery. Fairly large hepatic injuries may be missed without intravenous contrast enhancement. Conversely, small hematomas may be visible as densities on a non-contrast scan (and obscured by contrast-enhanced parenchyma). These are usually not clinically significant and preliminary non-contrast CT may be safely omitted when you are pressed for time. If non-operative management is chosen, CT or sonography can be used for follow-up. The liver injuries likely to be encountered on CT include contusions, subcapsular and parenchymal hematomas, lacerations and fractures. Contusions are ill-defined intraparenchymal lucencies. Subcapsular hematomas are lenticular lucent peripheral collections that indent the liver contour. Intraparenchymal hematomas are rounded or slightly irregular lucent collections. Fresh and clotted blood is hyperdense on non-contrast scans as opposed to its hypodense appearance after contrast. Lacerations are linear, sometimes branching radiolucencies, referred to as burst injuries when complex and extensive. When a laceration avulses a segment or lobe it is called a fracture.
Potential complications that should be sought during follow-up of a conservatively treated hepatic trauma patient or a postoperative patient include: arterial pseudoaneurysm (angiography and Doppler sonography are helpful additional studies), intra- or perihepatic abscess, biloma or biliary fistula. Radionuclide hepatobiliary scintigraphy is a sometimes helpful noninvasive adjunctive study for the latter two conditions.