
Інші зображення цього випадку

Image
Chance Fracture
- Image ID
- MPX2376_synpic33071
- Case U_id
- MPX2376
- Modality
- MR · MR - T1W - noncontrast
- Plane
- Lateral
- Location
- Spine (Spine and Muscles)
- Age / Sex
- 21 / male
- Caption
- MRI shows increased intensity at T11, characteristic of blood and edema in this area, suggestive of a Chance Fracture.
- ACR Codes
- 3.4
Clinical case
- History
- 21 year old man with back pain after a motor vehicle accident.
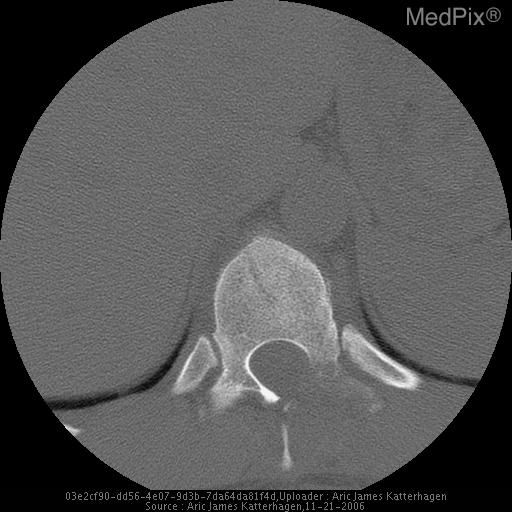
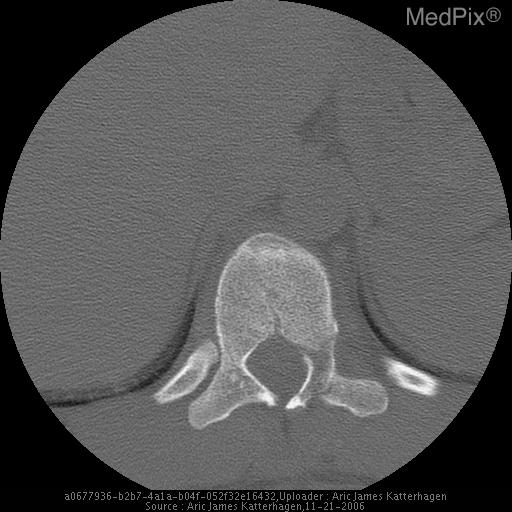
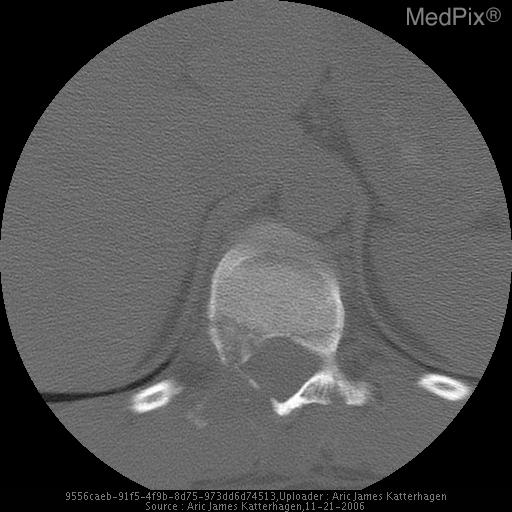
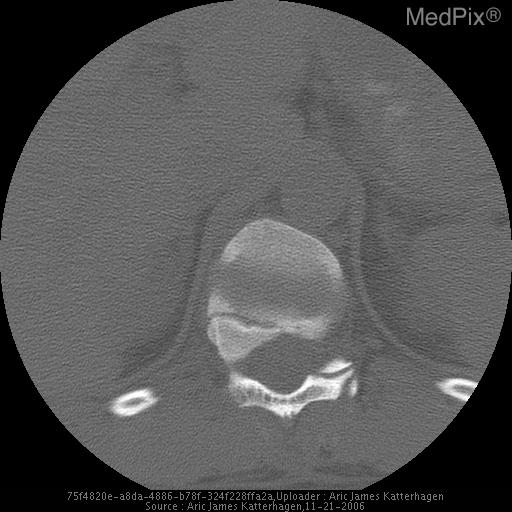
- Findings
- T11 Fracture of vertebral body, posterior elements, and widened interspinous space T11 abnormal Hyperintense signal and compression on T1 MRI
- Differential Diagnosis
- Wedge Fracture Chance Fracture Compression Fracture
- Case Diagnosis
- Chance Fracture
- Diagnosis By
- CT / MRI
Topic
- Category
- Trauma
- ACR Code
- 3.4
Disease discussion
Chance fractures, first described by G.Q. Chance in 1948, are horizontal vertebral fractures that extend through the vertebral body, pedicles and to the spinous process or lamina. The plain films are characteristic of wedge compression fractures while the posterior components are displaced to varying degrees. The posterior displacements are often better visualized on MRI and more specifically CT. CT with sagittal reconstructions are recommended.
Chance fractures commonly occur at the thoracic/lumbar junction where the spine transitions from a rigid to a more flexible segment. The etiology of these fractures is most often hyperflexion of the back. With the increasing use of lap seat belts in the 1950s-70s these fractures became known as “seat belt” fractures as vehicle accidents would cause sudden flexion of the waist at the thoracic/lumbar junction inducing significant stress on the posterior column. With the addition of shoulder belts these injuries have become significantly less common. Most Chance fractures seen today are a result of falls or crush type injuries where the spine is acutely hyperflexed. Intraabdominal injuries are likely in approximately 50% of chance fractures so vigilance should be given to a thorough evaluation involving a CT of the abdomen.
Most Chance Fractures are managed with immobilization. Instability is frequently associated with a kyphosis of 20° or more and a kyphosis of 30° or more usually requires internal stabilization. Main treatment for unstable fractures is surgical fixation with spinal canal decompression.