Інші зображення цього випадку

Image
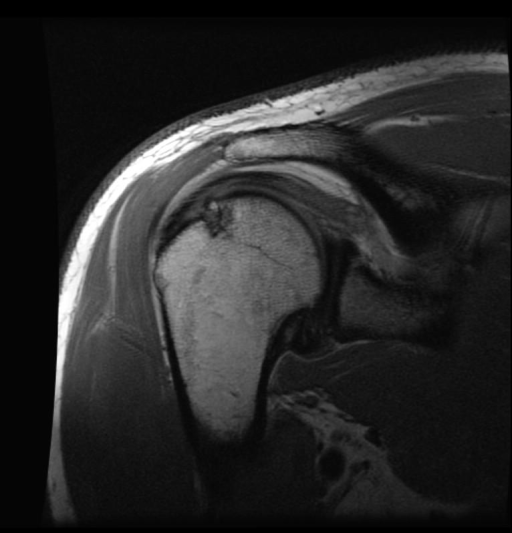
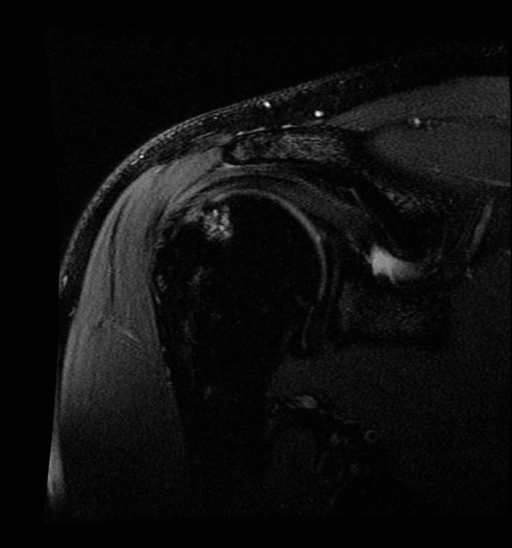
Hill-Sach’s lesion with underlying subcortical bone contusion and subchondral cyst formation consistent with chronicity.
- Image ID
- MPX2367_synpic24363
- Case U_id
- MPX2367
- Modality
- MR · MR - T1W - noncontrast
- Plane
- Axial
- Location
- Musculoskeletal (Spine and Muscles)
- Age / Sex
- 42 / male
- Caption
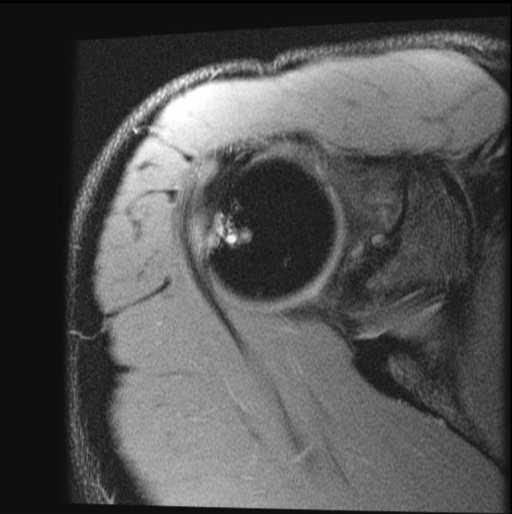
- Axial proton-density with fat saturation MR image of the right shoulder shows an area of high signal intensity of the posterolateral humeral head and of the overlying cartilage consistent with a Hill-Sach's lesion.
- ACR Codes
- 4.3
Clinical case
- History
- 42 yo man presents with onset of right shoulder pain for two years, combined with right upper extremity numbness and tingling.
- Exam
- On physical exam there is no obvious deformity of right upper extremity and the shoulder girdles are symmetrical with normal contours. Pain in right upper extremity, with palpation internal and external rotation, and with passive and active range of motion. Special tests: Negative sulcus sign, positive apprehension test. No neurological deficits noted.
- Findings
- A-P radiograph of the right shoulder in internal rotation shows a grooved defect in the posterolateral humeral head. Axial proton-density with fat saturation MR image shows an area of high signal intensity of the posterolateral humeral head and overlying cartilage consistent with a Hill-Sachs lesion. Proton-density and the T2-weighted with fat sat coronal oblique MR images show the Hill-Sach’s lesion of the humeral head with fractured cortex. T2-weighted with fat sat sagittal oblique MR image shows the high signal intensity edema and subchondral cyst formation in humeral head beneath the Hill-Sach’s fracture. There is no evidence of bony Bankart lesion on the plain radiographs or bony or cartilaginous Bankart lesion on the MR images.
- Differential Diagnosis
- The findings are typical for Hill-Sach’s lesion.
- Case Diagnosis
- Hill-Sach’s lesion with underlying subcortical bone contusion and subchondral cyst formation consistent with chronicity.
Topic
- Category
- Trauma
- ACR Code
- 4.4
Disease discussion
A Hill-Sach’s lesion occurs when the humeral head is dislocated anterolaterally and impacts against the anterior glenoid bony labrum. This lesion can be seen in approximately 30-40% of patients who have first-time anterior dislocations and approximately 80% of patients with repeat dislocations. A Bankart lesion, which is defined as an avulsion of the anterior inferior glenoid labrum at its attachment to the inferior glenohumeral ligament complex, can accompany the Hill-Sach’s lesion. For patients with a Bankart lesion, 75% will also sustain a Hill Sach’s lesion. The probability of a recurrence is related to the age of the patient at time of injury. Recurrence of dislocations develops in 90% of patients under age 20 years, 60% of patients between 20 and 40 years, and 10% in patients over 40 years. The type of sporting activity (i.e. contact versus individual) and the level of sport participation (i.e. recreational versus professional) is also related to recurrence. For both lesions males are affected much more often than females, especially active adolescents and adults who are younger than age 25. However, as young women become more involved with athletics, the incidence of dislocations may change. Ethnicity of the patient is not a predisposing factor for dislocations. Although plain radiographs should always be the first study done to evaluate patients with any shoulder pain, MR imaging is the procedure of choice to diagnose and define the extent of the lesion. In fact, MR imaging resulted in a sensitivity of 97%, a specificity of 91%, and an accuracy of 94% in the detection of Hill-Sach’s lesions. T2-weighted MR images will show high signal intensity at the site of impaction of the humeral head. T2-weighted MR images may also show subcortical bone high signal intensity that represents an area of contusion or subchondral cyst formation when chronicity is present.