Інші зображення цього випадку
Image
Osteochondritis dissecans
- Image ID
- MPX2351_synpic45942
- Case U_id
- MPX2351
- Modality
- MR · MR - T1W - noncontrast
- Plane
- Coronal
- Location
- Musculoskeletal (Spine and Muscles)
- Age / Sex
- 35 / male
- Caption
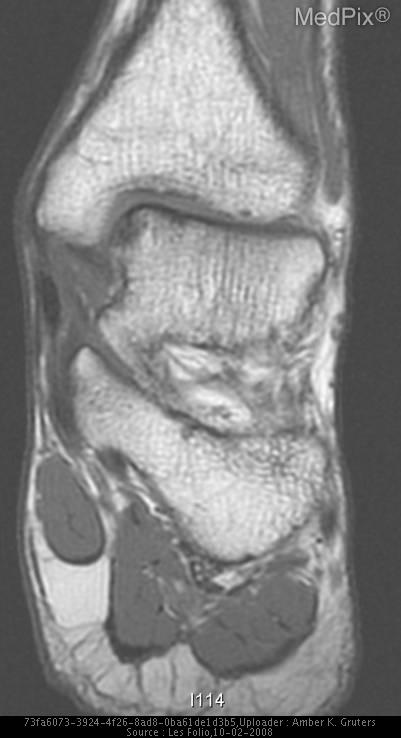
- T1-weighted MR image shows focus of low signal intensity in the medial aspect of the left talus.
- ACR Codes
- 4.4
Clinical case
- History
- 35 year old active duty Air Force male nordic skiier (National Ski Patrol European Division) who was training for advanced mountaineering expeditions on the Concordia Glacier presents with ankle pain.
- Exam
- The patient has point tenderness on the talus and has 12 degrees of pronation bilaterally. He has a history of multiple fractures of the left foot to include a Jones fracture and a navicular fracture. He has disregarded medical advice for post-trauma care in the past. For example, he began water skiing only three weeks after two fractures of the foot with refusal of a cast.
- Findings
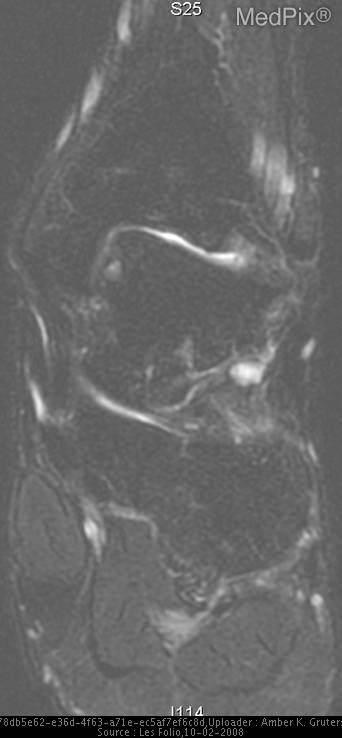
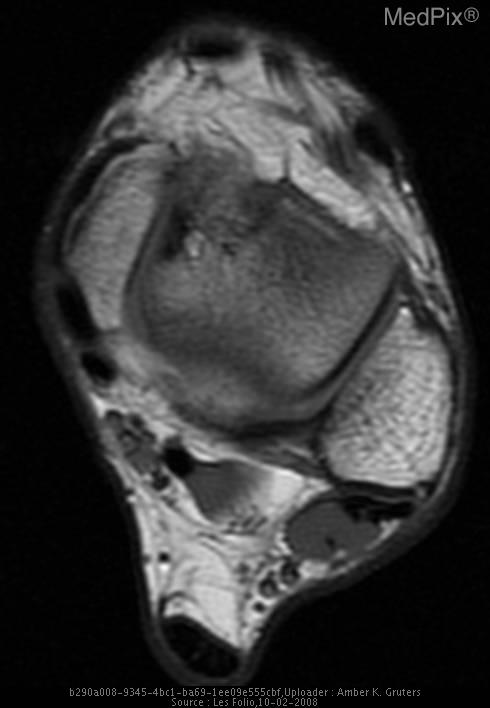
- AP and lateral radiographs of left ankle are negative. T1-weighted MR image shows focal area of low signal intensity in the medial aspect of the left talus. FSE T2-weighted MR image with fat saturation shows focal area of high signal intensity in the anteromedial aspect of the left talus.
- Differential Diagnosis
- Osteochondritis dissecans Osteochondral fracture Acute stress fracture
- Case Diagnosis
- Osteochondritis dissecans
- Diagnosis By
- Diagnosis confirmed by radiographic findings and patient history of repetitive trauma.
Topic
- Category
- Trauma
- ACR Code
- 4.4
Disease discussion
Osteochondritis dissecans (OCD) is believed to result from repetitive microtrauma. The initial trauma is an acute osteochondral fracture. The knee is involved in 75% of all patient presentations. It is most common in young male athletes, with a male:female ratio of 2-3:1. It is rarely seen in patients younger than 10 years of age or older than 50 years. There are two forms of OCD, the juvenile form affects children with open physes between the ages of 5 to 15 years. The adult form is present in patients with closed physes.
With OCD of the talus, patients present with complaints of ankle "catching" with active motion or walking. They may have swelling or pain depending of the stage of lesion. On physical examination, patients may have diffuse or well-defined tenderness with a joint effusion, pain with tibiotalar joint compression, and/or crepitus with dorsiflexion or plantar flexion.The cartilaginous and subchrondral bone lesions are usually on the posteromedial or the anterolateral talar aspect.
OCD of the talus is likely due to trauma causing tibiotalar subluxation with subsequent impingement of the talus on the tibia or fibula. Berndt and Harty observed in cadavers that impaction of the talus on the fibula in inversion with the ankle positioned in dorsiflexion results in anterolateral talar lesions. Posteromedial lesions could be created after inversion with a plantar-flexed ankle with resulting talus impaction and twisting on the posterior aspect of tibia.
Radiographs may be adequate for diagnosis but they may also show no findings. Radiographs should always be obtained, but if negative, an MRI should be done for confirming the suspected clinical diagnosis when necessary. AP, lateral, and mortise radiographs are the standard radiologic images. Berndt and Harty's radiographic classification of OCD of the talus is used for determining the type of treatment and the prognosis. Stage I is a small area of compression of subchondral bone. Stage II is a partially detached osteochondral fragment. Stage III is a completely detached fragment that remains in underlying bone depression. Stage IV is a completely detached fragment with displacement from the subchondral bone depression.
Canale and Belding recommend the following for all Berndt and Harty talar lesions:
Stage I and II - conservative treatment and protected weight-bearing
Stage III anterolateral – operative debridement and curettage
Stage III posteromedial –immobilize limb in cast or brace and no weight-bearing for six months
Stage IV - operative debridement and curettage