Інші зображення цього випадку


Image
Quadriceps tendon rupture, Medial retinacular tear
- Image ID
- MPX2204_synpic23796
- Case U_id
- MPX2204
- Modality
- MR · MR - T1W - noncontrast
- Plane
- Axial
- Location
- Musculoskeletal (Spine and Muscles)
- Age / Sex
- 48 / male
- Caption
- Quadriceps tendon rupture;Medial retinacular tear
- ACR Codes
- 4.4
Clinical case
- History
- 48 y/o male presents with pain in anterior aspect of distal right thigh, superior to right knee and increased pain in right knee. The patient has had knee pain for two years that limited his ability to run.
- Exam
- Physical Exam and Laboratory: Physical examination shows a large deep palpable defect in the soft tissues in the anterior aspect of right thigh, superior to the patella. The patient was unable to extend his right leg. No laboratory data are available.
- Findings
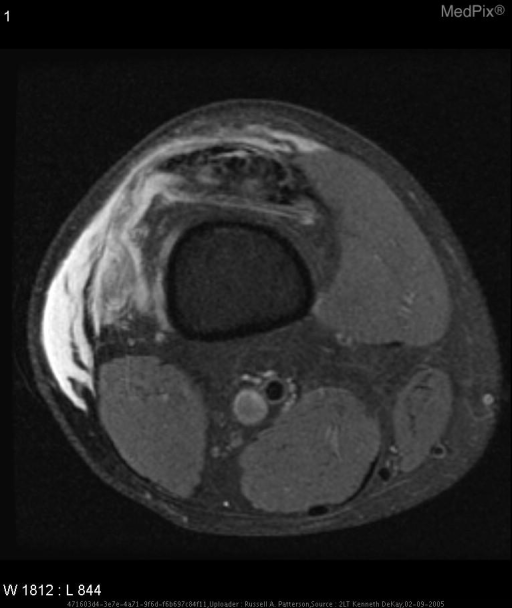
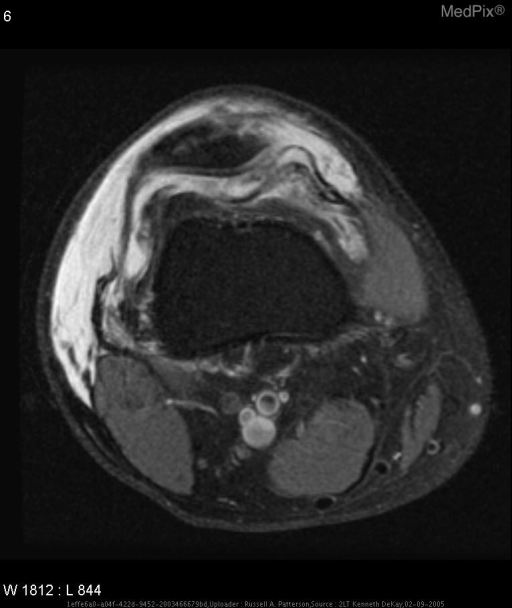
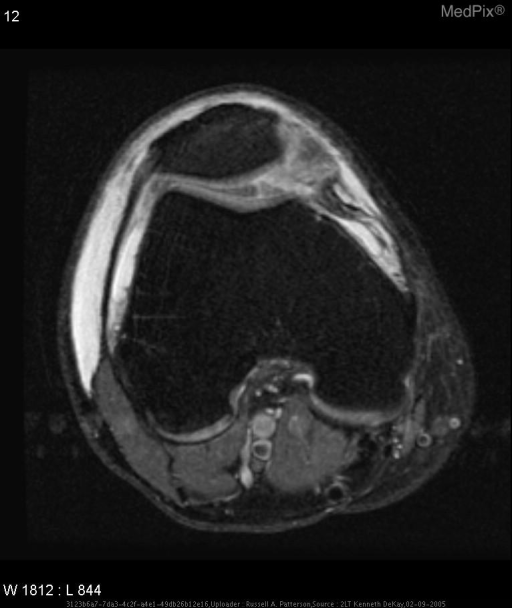
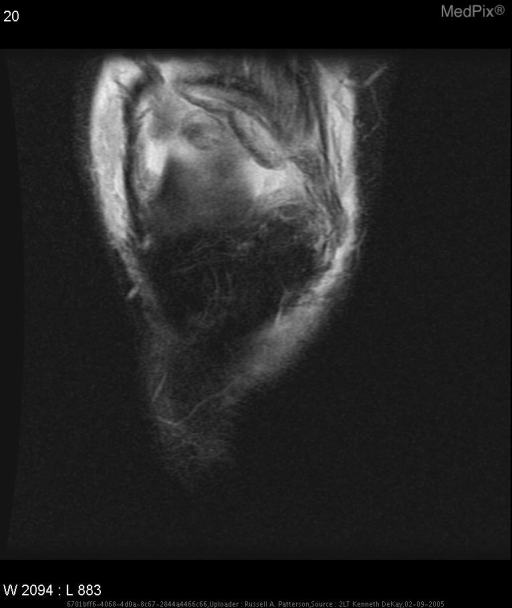
- Lateral radiograph of the knee shows patella baja. Proton-density and gradient-recalled echo sagittal oblique MR images show a complete tear of the quadriceps tendon with high-signal-intensity hemorrhage/edema filling the gap. Separation of the tibial tuberosity without associated edema suggest old Osgood-Schlatter’s disease. T2-weighted fat sat axial images from the level of the distal femoral diaphysis to the femoral condyle show the quadriceps tendon tear with high signal intensity, the tear of the medial retinaculum at its attachment site to the patella with medial and posterior displacement of torn fibers and extensive high-signal-intensity edema/hemorrhage in the soft tissues particularly laterally. A post traumatic chondral defect with subchondral edema was also seen within the medial patellar facet (image not included).
- Differential Diagnosis
- Quadriceps tendon rupture Medial retinacular tear
- Case Diagnosis
- Quadriceps tendon rupture, Medial retinacular tear
- Diagnosis By
- At surgery.
Topic
- Category
- Trauma
- ACR Code
- 4.4
Disease discussion
Discussion (include references): The mechanism of injury that causes quadriceps rupture is trauma, although this injury can also occur spontaneously. In the setting of trauma, it can either be direct or indirect. Direct trauma results from a direct blow to the quadriceps muscle, causing it to tear. An indirect injury is caused by a rapid and severe contraction of the quadriceps while the knee is in flexion. Both of these mechanisms can cause complete or partial tears. Spontaneous injury usually occurs in the elderly and is often associated with chronic diseases (although it can happen in healthy individuals) such as diabetes mellitus, renal failure, systemic lupus erythematosus, rheumatoid arthritis, or gout. It has also been associated with corticosteroid therapy. Most tears will occur at the quadriceps enthesis and distal quadriceps tendon near its insertion side into the patella. Medial and lateral retinacular tears occur when there is valgus or varus angulation while the quadriceps is contracted.
On physical exam a partial tear can be difficult to discern. The findings will include decreased extension strength that is often only evident only when done against resistance. Complete tears are much easier to observe. Examination will elicit inability to extend the knee, soft tissue hematoma, or a palpable/visible gap in the soft tissue superior to the patella. Studies that are done to support the physical findings should include radiographs followed by sonography when patellar subluxation is not present, and magnetic resonance imaging (MRI).
On routine radiograph, findings that are associated with a complete tear are soft tissue swelling, inferior positioning of the patella (also known as patella baja), distortion of the soft tissue planes above the patella, and avulsed patellar fragments. If there is no other injury suspected other than the quadriceps tendon rupture and no subluxation of the patella, sonography, sonography is a useful and inexpensive test to confirm the radiological findings. However, sonography does not allow an adequate evaluation of the osseous and cartilaginous structures and other ligaments such as retinacula and collateral ligaments. When other abnormalities are suspected,. MRI should be performed after the plain radiographs. On MR images, a complete tear will appear as disruption of the low-signal-intensity tendon with high-signal-intensity hematoma/ post-traumatic inflammation filling the gap of the torn tendon. MRI also confirms the patella baja. The tear should be evaluated in three planes for its full extent. MRI also demonstrates associated injuries such as medial retinacular tear, with the disruption of the retinaculum usually at its patellar insertion and an infolding of the retinaculum medially and even posterior to the tendon. Hematomas of the soft tissue and patellar avulsions and contusions, and osteochondral trauma can also be shown.
When identified, the quadriceps rupture should be treated expeditiously. When the injury is complete as in this case, direct end to end repair is done with immobilization of the knee in extension. The repair shows the best results when done within two months of the injury. With delay in treatment, proximal migration and scarring of the quadriceps occurs and surgery more difficult, sometimes requiring the quadriceps lengthening procedures, a muscle or tendon transplant or both.