
Інші зображення цього випадку

Image
Calcaneal Stress Fracture
- Image ID
- MPX2066_synpic26220
- Case U_id
- MPX2066
- Modality
- MR · MR
- Plane
- Coronal
- Location
- Musculoskeletal (Spine and Muscles)
- Age / Sex
- 18 / male
- Caption
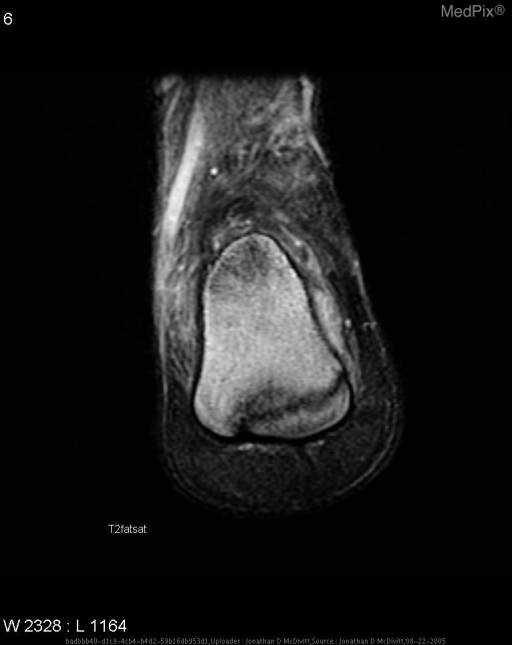
- Coronal MR T1
- ACR Codes
- 4.4
Clinical case
- History
- 18 y/o male undergoing military boot camp who complains of right ankle pain upon jumping out of bed (approximately 6 ft high fall) and landing on ankle.
- Exam
- Patient complained of point tenderness upon palpation of ankle. Rest of physical noncontributory.
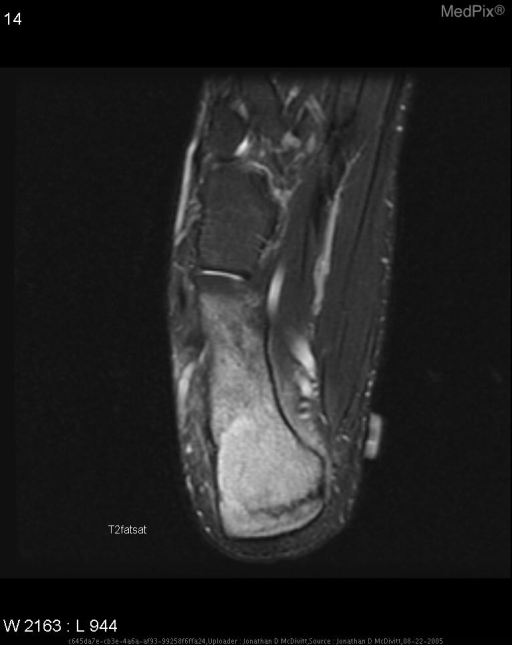
- Findings
- Plain Films: No acute findings MRI: Nondisplaced, compression type fracture of posterior calcaneus with extensive bone marrow and surrounding soft tissue edema.
- Differential Diagnosis
- -Ankle Sprain -Stress Fracture -Arthritis -Tenosynovitis
- Case Diagnosis
- Calcaneal Stress Fracture
- Diagnosis By
- Radiographically
Topic
- Category
- Trauma
- ACR Code
- 4.4
Disease discussion
Stress fractures are classified into either fatigue or insufficiency type fractures. Fatigue type fractures result from the application of unusual force/torque onto a normal bone, this is common among athletes (especially long distance runners or ballet dancers) or in military members (especially recruits in basic training or undergoing parachute training). Insufficiency type fractures results from the application of normal stress on an abnormal bone. The underlying abnormality of the bone arises from a diverse array of causes, including osteoporosis, Paget's disease, osteomalacia, hyperparathyroidism, renal osteodystrophy, rheumatoid arthritis, fibrous dysplasia, irradiation, and so forth.
Clinically the patient complains of activity-related pain that is relieved by rest. There also may be a localized soft tissue swelling or tenderness, though the specific site and activity being engaged in influences these variables.
The most common site of fatigue-type stress fractues is the metatarsals (march fracture) with the second most frequent location being the calcaneus. These calcaneal stress fractures are usually found with a vertical or oblique orientation in the posterior or posterosuperior portion of calcaneus. Radiographs are often normal initially though MR and bone scan offer increased sensitivity and can be used with a high index of clinical suspsion even if the plain radiograph is normal.