Інші зображення цього випадку
Image
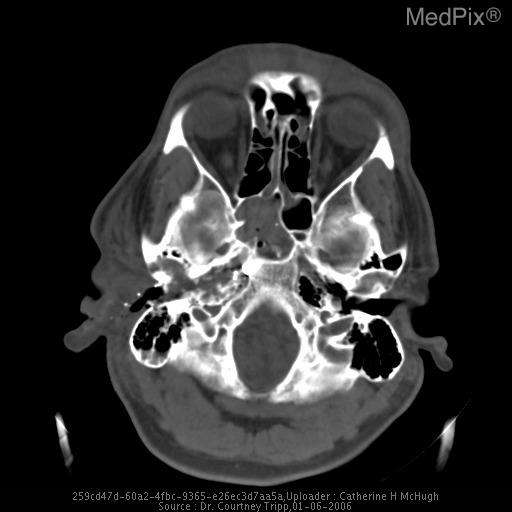
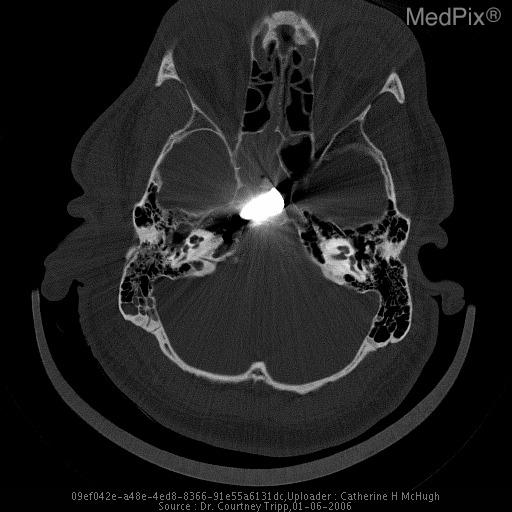
Bullet to the clivus.
- Image ID
- MPX2060_synpic27727
- Case U_id
- MPX2060
- Modality
- CT · CT - noncontrast
- Plane
- Axial
- Location
- Generalized (Head)
- Age / Sex
- 35 / male
- Caption
- Soft tissue windows showing entrance wound
- ACR Codes
- 9.4
Clinical case
- History
- A male soldier was shot in the right shoulder while on security detail in Iraq.
- Exam
- Entrance and exit wound in right shoulder. Also entrance wound in Right EAM. Not able to hear out of right ear.
- Findings
- Metallic fragments from projectile in right temporal bone demonstrating ballistic tract. The bullet entered the external auditory canal, penetrated the petrous portion of the temporal bone, and stopped in the clivus. The bullet appears to have tumbled from when it entered the EAM to lodging into the clivus.
- Differential Diagnosis
- Bullet to the clivus.
- Case Diagnosis
- Bullet to the clivus.
- Diagnosis By
- CT only, bullet was left in.
Topic
- Category
- Trauma
- ACR Code
- 9.4
Disease discussion
In ballistic trauma it is important to account for all bullets, whether lodged in the patient’s body or exited through a wound. The even # rule, as discussed below, is a useful tool to quickly account for all foreign bodies that have entered a patient. Even # rule deviation should prompt the physician to initiate further investigation to locate the discordant bullet(s) or come up with another explanation (i.e. shared exit wound).
EVEN # RULE
• Entrance + exit + bullet = even # (all bullets accounted for)
Any of the following may occur:
– all bullets exited
– all bullets lodged in body tissue
– all bullets exited or lodged in body tissue
• If entrance + exit + bullet = an odd # then not all bullets are accounted for, hence further imaging or explanation necessary
– shared exit wound
– bullet embolization
BULLET EMBOLISM
Bullet embolism is a rare complication of vascular trauma. When a firearm missile enters a vascular structure, the projectile can pass through both walls of the vessel or settle within the wall or lumen. If the latter occurs, the missile may be carried by the flow of blood to a new site resulting in an embolism (1,2,3).
Symptomatic arterial emboli may result in peripheral ischemia and should be removed quickly to avoid tissue or neurologic damage. Asymptomatic, cerebral, pulmonary, and pelvic arterial emboli may remain in place, especially if removal is technically difficult (3). Possible adverse effects of this decision, however, may lead to further embolization or migration, thrombosis, potential delayed arterial insufficiency, and subsequent pseudoaneurysm.
The Lodox Statscan™ (see related links) allows for total body imaging in a short period of time for quantifying multiple projectiles.