
Інші зображення цього випадку


Image
meniscal tear
- Image ID
- MPX1909_synpic16189
- Case U_id
- MPX1909
- Modality
- MR · MR - Other Pulse Seq.
- Plane
- Sagittal
- Location
- Musculoskeletal (Spine and Muscles)
- Age / Sex
- 26 / male
- Caption
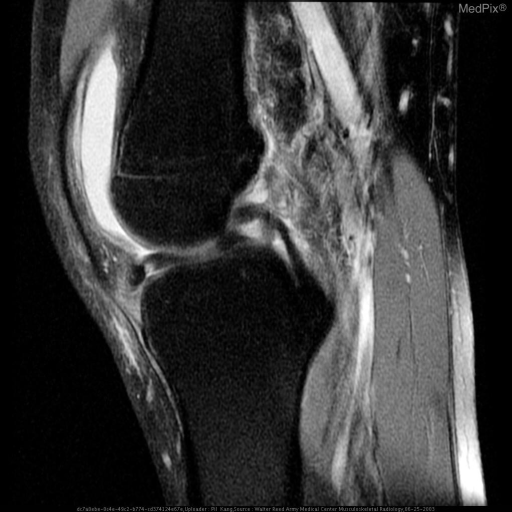
- Multiple sagittal MR sequence images demonstrate a tear of the medial meniscus with a displaced fragment in the intercondylar notch, in the classic "double PCL" sign, suggestive of a bucket handle tear.
- ACR Codes
- 4.4
Clinical case
- History
- 26 y.o. male injuried in weekend football game
- Exam
- N/A
- Findings
- Multiple sagittal MR sequence images demonstrate a tear of the medial meniscus with a displaced fragment in the intercondylar notch, in the classic "double PCL" sign, suggestive of a bucket handle tear.
- Differential Diagnosis
- bucket handle tear of medial meniscus
- Case Diagnosis
- meniscal tear
Topic
- Category
- Trauma
- ACR Code
- 4.4
Disease discussion
Vertical longitudinal tears or bucket-handle tears make up 10% of all meniscal tears. MR imaging characteristics include: 1) "absent bowtie sign", where only one instead of the normal two body segments present on the outermost sagittal images; 2) "double PCL sign", where the displaced fragment of the tear is found in the intercondylar notch just anterior to the posterior cruciate ligament; 3) "anterior flipped meniscus sign", where the tear fragment flip over the anterior horn of the affected meniscus. (1)
Menisci in the knee are C-shaped, fibrocartilagenous structures with thick periphery and thin central portions. Vascularity of the meniscus is greatest near the periphery (near its attachment to the joint capsule) and is almost non-existent near the free edge. (1)
According to current orthopedic surgery literature, meniscus tears known to be suitable for repair with high expectation for success are traumatic lesions within the vascular zone in which the peripheral circumferential fibers remain intact and there is minimal damage to the meniscus body. Tears should generally be greater than 8mm, as shorter tears are more likely to heal spontaneously and even if they persist are likely to be asymptomatic. The most common tear types that fit these criteria: peripheral or near peripheral, vertical, or longitudinal tears. Those tears that are questionable in terms of being surgical candidates are those which are in avascular portion of the meniscus or when vascularity is in question, complete radial tears at the meniscosynovial junction, and tears that result in extensive damage to the body. (2)