Інші зображення цього випадку
Image
Bronchopleural Fistula
- Image ID
- MPX1674_synpic34452
- Case U_id
- MPX1674
- Modality
- CT · CT w/contrast (IV)
- Plane
- Axial
- Location
- Chest, Pulmonary (Thorax)
- Age / Sex
- 26 / male
- Caption
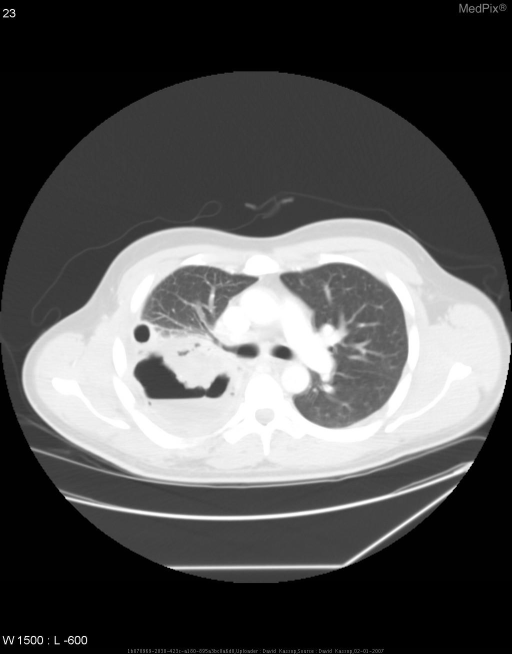
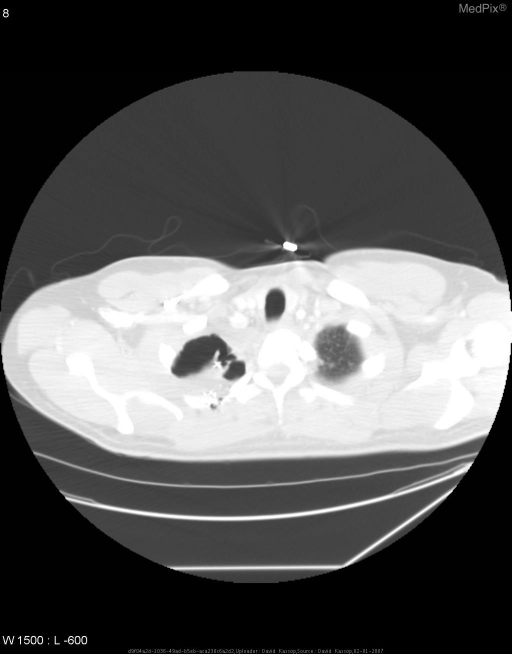
- Within the right hemithorax, there is a persistent moderate sized pleural effusion with a focal area of fluid at the right lung apex with an internal air fluid level consistent with loculated hydropneumothorax. Along the anterior aspect of this focal fluid collection there is soft tissue density material with internal air bronchograms as well as heterogeneous low density material which may represent an infarcted portion of the right upper lobe. A prior chest tube tract is appreciated along the anterior lateral aspect of the right thorax. Interval increase in size of the patient’s right apical subcutaneous emphysema as well as increased size of the patient’s right hydropneumothorax consistent with bronchopleural fistula with continued communication to the subcutaneous tissues likely via the posterior apical comminuted rib fractures. Findings also suggestive of lung infarction involving the posterior aspect of the right upper lobe.
- ACR Codes
- 6.4
Clinical case
- History
- 26 y.o. returning from Operation Iraqi Freedom s/p GSW to right chest three weeks ago - now presenting with fevers, chills, night-sweats, and painful, non-productive cough overnight.
- Exam
- Physical exam was significant for the following: -Lungs: Symmetric chest expansion with decreased breath sounds throughout right lung fields and faint crackles in the right lung base. -Cardiac: Tachycardic; no murmurs/rubs/gallops Lab findings were significant for the following: WBC count of 19.1 and rising.
- Findings
- • CXR1: At the right lung apex, there is a prominent air-fluid level with post-traumatic changes. There is subcutaneous air within the right neck. Shrapnel overlies the midline and surgical clips are noted at the right lung apex. These findings are consistent with right hydropnemothorax. Also, with noted subcutaneous air over the right neck, these findings altogether make this concerning for bronchopleural fistulous formation between the right pleural space and the subcutaneous tissues of the right neck. • CXR2: There is a moderate sized right apical pneumothorax with air fluid level within the mid portion of the right hemithorax consistent with a hydropneumothorax. There is opacification along the right lateral thoracic wall with additional right basilar opacification. Again, there is a large subcutaneous collection of air along the soft tissues overlying the right apex. Also noted are multiple riht apical posterior rib fractures unchanged from previous films. Persistent opacification along the lateral aspect of the right lower lung and along the right lung base is consistent with tracking pleural fluid and adjacent atelectasis. • CT scans: Within the right hemithorax, there is a persistent moderate sized pleural effusion with a focal area of fluid at the right lung apex with an internal air fluid level consistent with loculated hydropneumothorax. Along the anterior aspect of this focal fluid collection there is soft tissue density material with internal air bronchograms as well as heterogeneous low density material which may represent an infarcted portion of the right upper lobe. A prior chest tube tract is appreciated along the anterior lateral aspect of the right thorax. Interval increase in size of the patient’s right apical subcutaneous emphysema as well as increased size of the patient’s right hydropneumothorax consistent with bronchopleural fistula with continued communication to the subcutaneous tissues likely via the posterior apical comminuted rib fractures. Findings also suggestive of lung infarction involving the posterior aspect of the right upper lobe.
- Differential Diagnosis
- Bronchopleural fistula Hydropneumothorax with subcutaneous emphysema
- Case Diagnosis
- Bronchopleural Fistula
- Diagnosis By
- Video-Assisted Thoracic Surgery (VATS)
Topic
- Category
- Trauma
- ACR Code
- 6.4
Disease discussion
Bronchopleural Fistula
Bronchopleural Fistulas (BPFs) are communications between the pleural space and the bronchial tree. They are relatively rare but a feared complication of several pulmonary conditions. They have a high morbidity and mortality rate, associated with a prolonged hospital stay, and result in high resource utilization. The incidence of BPF has been reported from 1.5 to 28% after pulmonary resection. This patient’s BPF is a result of penetrating trauma that over time caused necrotizing lung to form a fistula. As a result, the patient’s subcutaneous emphysema was able to increase in size rather quickly. Additionally, tracking pleural fluid is able to accumulate as well. After the chest x-ray and CT scan of the chest, the patient was started on broad-spectrum antibiotics and had a right chest tube placed. Later that morning, the patient was taken for Video-Assisted Thoracic Surgery for drainage and surgical closure of the fistula. The patient did not have any intraoperative complications and is currently recovering.