Інші зображення цього випадку



Image
Bilateral pleural effusions, bilateral pelvic hematomas, fracture/tract of left iliac, Left 5th rib fracture, thickening of gastric wall - non-specific changes, and post surgical changes to left upper quadrent status post splenectomy.
- Image ID
- MPX1519_synpic31540
- Case U_id
- MPX1519
- Modality
- CT · CT w/contrast (IV)
- Plane
- Axial
- Location
- Generalized (Abdomen)
- Age / Sex
- 25 / male
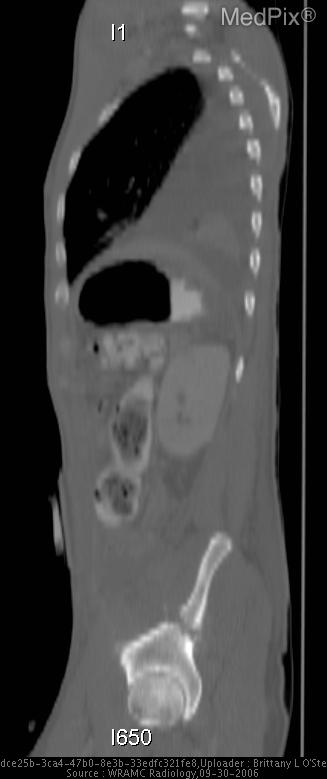
- Caption
- Fracture of left rib which follows one of the entrance tracts.
- ACR Codes
- -1.-1
Clinical case
- History
- 25 y/o man with 3 GSW to chest, abdomen, and Left buttock. Pt was resuscitated and had an ex-lap performed before transfer to WRAMC.
- Exam
- HR 116/65, P 85, RR 16, T 97.6. AOx3, equal BS with no rales, rhonchi, or wheezes. 3 cm chest wall wound tracking under subcutaneous tissue inferiorly. Abdomen is soft, NT, ND. Midline incision with staples, no erythema, purulence, or tenderness. LLQ end colostomy with stoma in place. Less than 1 cm entrance wound on the left buttock with no signs of purulence or erythema. No neurological deficits noted.
- Findings
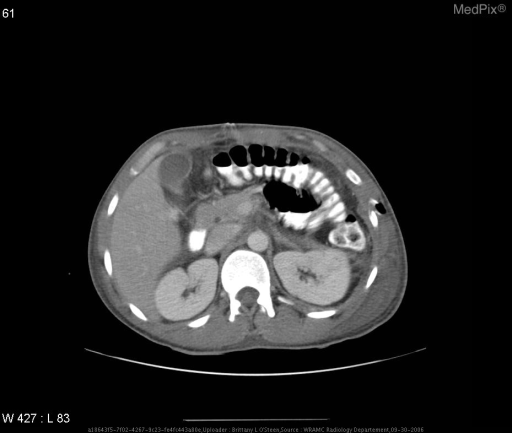
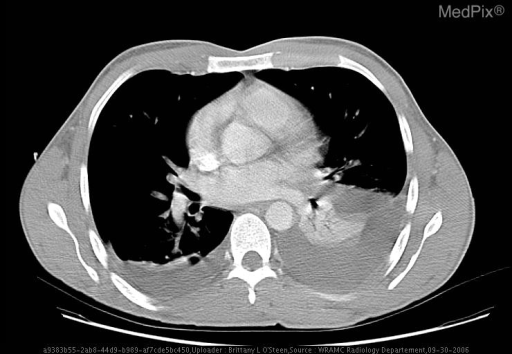
- Chest film: Blunting of CP angles especially on left. Air bronchograms and atelectatic lungs. Positive spine sign. CT: Bilateral pleural effusions with compressive attelectasis L>R. Multiple prominent axillary lymph nodes are identified meeting pathologic criteria in number but not in size. A hypodense band is seen in the upper pole of the left kidney representing laceration. Post surgical changes are noted in the L upper abdomen with 2 metallic clips seen and an absent spleen. Clip is in the L hemidiaphragm status post diaphragmatic rupture. Colostomy is seen on left with descending colon attached. The stomach reveals a thickened and irregular wall with out evidence of a filling defect or focal mass. Two fluid collections are seen in the pelvis, one in the left hemipelvis anterior to the iliac and the second in the right hemipelvis consistent with hematomas. Air can be seen in the left gluteus maximus and in the left lateral wall representing bullet tract. In the bony structures there is a complete fracture through the wing of the left ilia with several bone fragments in the pelvis consistent with the ballistic tract. A fracture is also noted in the middle portion of the left 5th rib from another bullet.
- Differential Diagnosis
- PolyTrauma from multiple ballistics
- Case Diagnosis
- Bilateral pleural effusions, bilateral pelvic hematomas, fracture/tract of left iliac, Left 5th rib fracture, thickening of gastric wall - non-specific changes, and post surgical changes to left upper quadrent status post splenectomy.
- Diagnosis By
- Imaging, Findings from previous exploratory laparotomy
Topic
- Category
- Trauma
- ACR Code
- 4.4
Disease discussion
Typically, penetrating diaphragm injury is difficult to diagnose without a high index of suspicion. Penetrating diaphragm injuries (PDI) tend to be smaller than blunt diaphragm injuries. PDI’s typically are ≤1-2 cm in length. Diaphragm injuries are most easily diagnosed at laparotomy but not all patients have indications for an initial laparotomy.
In trauma, a chest radiograph is typically the first imaging modality employed. This can be helpful in the initial evaluation for inspecting the integrity of the hemi-diaphragms but patient positioning and the quality of portable films can limit their usefulness. Many patients with trauma ultimately undergo a CT study. Multiplanar reconstructed images have been reported by some to be helpful in detecting diaphragm injuries. There are fewer studies on the use of CT with PDI, one small study by Larici, et al. reported a sensitivity of 86% and a specificity of 79% of detecting PDI’s with helical CT.
Herniation of abdominal fat into the thorax is one sign that is commonly used to detect blunt diaphragm rupture can still be used when looking for PDI. The most specific sign of PDI is a wound tract that is found on both sides of the diaphragm. This has a reported specificity of 100% and a sensitivity of 36%. A hemothorax or wound tract near the diaphragm should heighten the radiologist’s suspicion for a diaphragm injury.