Image
Lipohemarthrosis (s/p BKA for IED & shrapnel injury)
- Image ID
- MPX1504_synpic49211
- Case U_id
- MPX1504
- Modality
- CT · CT - noncontrast
- Plane
- Axial
- Location
- Musculoskeletal (Spine and Muscles)
- Age / Sex
- 26 / male
- Caption
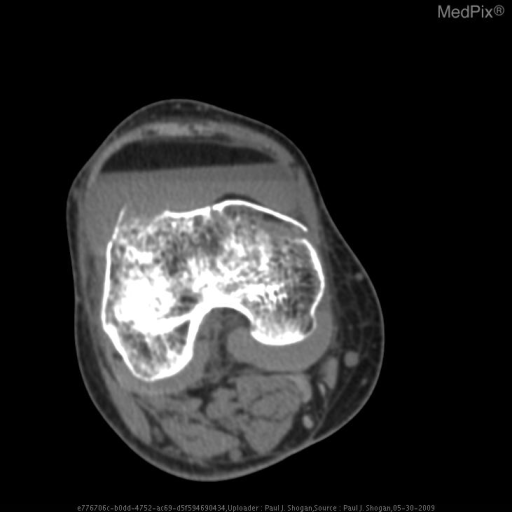
- Nonenhanced axial CT image in soft tissue windows through the level of the femoral condyles, shows the complex fracture with an associated joint effusion with three distinct layers: an anterior fat density layer, an intermediate fluid density layer, and a posterior hyperdense layer.
- ACR Codes
- 4.4
Clinical case
- History
- 26 year old man with with a swollen knee after falling. Past history of a below the knee amputation (BKA) five years ago.
- Findings
- AP radiograph of the right knee shows cortical irregularity at the superior aspect of the medial femoral condyle, and lateral aspect of the lateral femoral condyle. The patient is post BKA, with prior surgical changes noted in the proximal tibia and diffuse osteopenia. Heterotopic ossification and shrapnel are seen in the soft tissues. Lateral radiograph of the right knee shows a complex fracture of the distal femur, with cortical disruption of the medial femoral condyle and a 6 mm gap involving the lateral femoral condyle. A joint effusion is noted. The patient is post BKA, with prior surgical changes noted in the proximal tibia and diffuse osteopenia. Heterotopic ossification and shrapnel are seen in the soft tissues. Nonenhanced axial CT image in bone windows through the level of the femoral condyles, shows the complex fracture with an associated joint effusion with three distinct layers: an anterior fat density layer, an intermediate fluid density layer, and a posterior hyperdense layer. Nonenhanced axial CT image in soft tissue windows through the level of the femoral condyles, shows the complex fracture with an associated joint effusion with three distinct layers: an anterior fat density layer, an intermediate fluid density layer, and a posterior hyperdense layer. X-table lateral radiograph of the right knee shows interval placement of a partially imaged trans-tibial pin and reduction of the complex distal femoral fracture. The joint effusion again demonstrates three distinct layers: an anterior fat density layer, an intermediate fluid density layer, and a posterior hyperdense layer.
- Case Diagnosis
- Lipohemarthrosis (s/p BKA for IED & shrapnel injury)
- Diagnosis By
- Imaging findings are characteristic
Topic
- Category
- Trauma
- ACR Code
- -1.-1
Disease discussion
Lipohemarthrosis is the result of extruded bone marrow fat and blood into joint space following an intraarticular fracture [1]. First described in 1929 by Kling, Holmgren demonstrated the “fat-fluid” level radiographically in 1939 [1,2]. In 1942, Pierce et al. described a fat-fluid level, which had a fluid-fluid component and suggested that this phenomenon was the result of separation of blood into serum and cellular elements [2]. In 1996, Lugo-Olivieri et al. performed a retrospective review of 41 patients with tibial plateau fractures and found that joint effusions with fluid levels resulted from blood separating into cellular elements and supernatant serum, confirmed with CT or MR imaging. Lugo-Olivieri concluded that a single fluid-fluid level on radiographs in a post-traumatic knee did not necessarily reflect lipohemarthrosis, as hemarthrosis could appear similarly. They suggested that a double fluid-fluid level is a more specific finding for intraarticular fat and an underlying fracture.
Lipohemarthrosis is more common in fractures about the knee, but has been described in the shoulder, elbow, and hip fractures [1]. CT and MRI are more specific than radiography in evaluating the composition of the effusion, but sonography may also have a role [1]. The anterior layer on ultrasound will appear hyperechogenic because of the fat. On CT, this area will be fat-density, and will follow fat signal on all MR pulse sequences [1,2]. The supernatant layer will be anechoic on US, fluid density on CT, and follow simple fluid signal on all MR sequences [1,2]. The hemorrhagic cellular layer will appear hypoechogenic on sonography, hyperdense (50 – 70 HU) on CT, and produce intermediate signal on T1 and hypointense signal on T2-weighted images [1,2].