Image
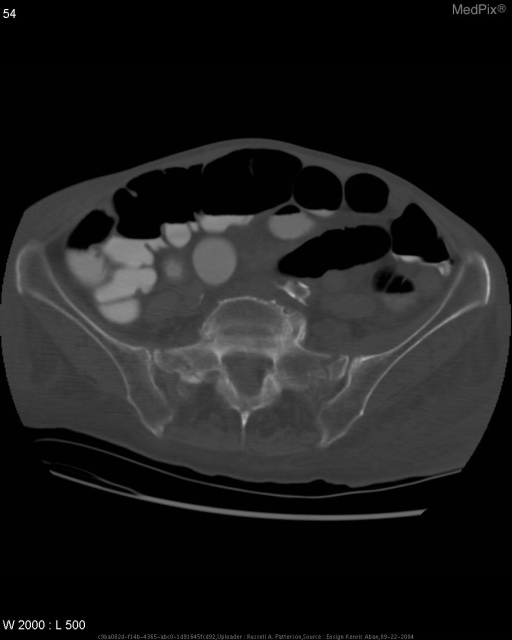
Bilateral sacral fractures
- Image ID
- MPX1432_synpic21430
- Case U_id
- MPX1432
- Modality
- CT · CT - noncontrast
- Plane
- Axial
- Location
- Musculoskeletal (Spine and Muscles)
- Age / Sex
- 77 / female
- Caption
- Bilateral sacral fractures
- ACR Codes
- 4.9
Clinical case
- History
- History (can include gestational age, or age in days, weeks, months):77 y/o Caucasian female with past medical history significant for Stage IIa bladder cancer treated with radiation therapy complaining of progressive left leg and hip pain that occurs while standing. Onset of pain and difficulty ambulating began just after her treatment for bladder cancer a few months ago. Over the last three weeks, she has lost the ability to walk without experiencing pain. Pain radiates from her left buttock to her knee and relieved when sitting, lying down, or using a heating pad. Patient has had two recent physical therapy visits, which provided notable relief but most recent visit provided no such relief. Patient also notes prior history of pain in her buttocks while walking. She has a questionable history of a fall a few weeks ago for which she did not seek medical care.
- Exam
- Phsical examination is positive straight leg raising test on the left
- Findings
- A-P radiograph of the pelvis can not adequately evaluate the pelvis secondary to obscuration by contrast-enhanced bowel. No hip fracture is seen.Axial CT of sacrum with bone windows shows shows bilateral sacral insufficiency fractures. Coronal reformatted CT of sacrum confirms bilateral sacral fractures.
- Differential Diagnosis
- Differential Diagnosis for these findings in this case:1. Insufficiency fracture secondary to radiation therapy2. Insufficiency fracture secondary to osteoporosis3. Fracture secondary to trauma
- Case Diagnosis
- Bilateral sacral fractures
Topic
- Category
- Trauma
- ACR Code
- 4.9
Disease discussion
Sacral fractures, especially insufficiency fractures in which stresses of normal activity are greater than the resistance ability of bone, are not uncommon in elderly women. Sacral fractures may be caused by high impact trauma or metastatic cancer or secondary to radiation therapy, steroid therapy, or osteoporosis. Several risk factors are associated with sacral insufficiency fractures, the most common being osteoporosis. However, rheumatoid arthritis, corticosteroid therapy, osteomalacia, Paget’s disease, osteogenesis, osteopetrosis, and fibrous dysplasia are also potential risk factors (1). Patients with sacral insufficiency fractures typically present with low back pain, buttock pain, groin pain, or hip pain. The most common site of sacral fractures is the sacral ala. The fractures typically course vertically parallel to the sacroiliac joints. Sacral insufficiency fractures are often times difficult to diagnose for several reasons. Findings on plainradiographs are subtle and may be overlooked due to obscuration of bony detail by bowel gas. Stress fractures are difficult to detect through cancellous bone in patients with osteoporosis. Another reason that this diagnosis is overlooked if the interpreter is not familiary with insufficiency fractures in the sacrum (2). The main radiographic evidence of such a fracture is sclerosis secondary to trabecular compression and callus formation. Additional studies may be performed to confirm the diagnosis. Computed tomography can accurately confirm diagnosis by demonstrating unilateral or bilateral fracture lines in the sacral ala parallel to the sacroiliac joints. With healing, the fracture lines become sclerotic. Magnetic resonance imaging demonstrates fracture lines as decreased areas of signal intensity on T1 weighted images. Bone scintigraphy commonly produces an H-pattern or butterfly pattern of increased signal uptake consistent with bilateral sacral fractures with vertical and horizontal fracture components (3).