Image
Sand Aspiration
- Image ID
- MPX1349_synpic45566
- Case U_id
- MPX1349
- Modality
- CT · CT - noncontrast
- Plane
- Axial
- Location
- Chest, Pulmonary (Thorax)
- Age / Sex
- 34 / male
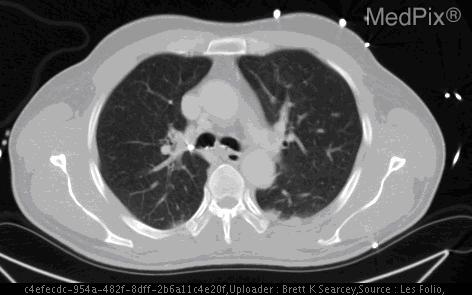
- Caption
- There is abnormal hyperattenuating material in the treacheobronchial tree.
- ACR Codes
- 6.4
Clinical case
- History
- A 34 year old man injured by a blast - he was facing the explosion when it went off.
- Exam
- He arrived with a Glasgow coma score of 15 and hypotensive. Physical exam on arrival revealed injuries consistent with the blast including multiple injuries to the face, left flank, back, left lower extremity, and an open distal tibia and fibula fracture with a retained foreign body. The bronchoscopy was notable for mild mucosal inflammation and a finding of yellow “mud” adherent to both the tracheal wall and the upper bronchi.
- Findings
- The chest x-ray was "negative" and is not included in this report. Chest CT imaging, obtained with the patient lying supine, revealed radiopaque material lining the dependant portions of the trachea as well as the main stem bronchi and bronchioles. No particulate matter was noted within the sinuses.
- Differential Diagnosis
- • Sand Aspiration • Drowning • Blast Lung
- Case Diagnosis
- Sand Aspiration
- Diagnosis By
- Bronchoscopy
Topic
- Category
- Trauma
- ACR Code
- 6.4
Disease discussion
Lesions/Condition: Sand Aspiration
Synonyms: Gravel Aspiration, Silt Aspiration
Associations/Predisposing Factors: Blast injury, Drowning, Near Drowning
The presentation of sand aspiration is highly variable. Certainly, sand visible within the oral cavity, oropharynx, or nasal passages can be indicative of sand aspiration in the correct clinical context. Clinical presentation can range from rapid death due to total occlusion of the airway and subsequent anoxic death to a spectrum of dyspnea, cough, and variable obstructive symptoms.1-4
In the past, the focus of reported radiographic imaging in sand aspiration has been on chest x-ray. Findings on chest roentgenograms may be highly variable, however Bonilla-Santiago described a characteristic “sand bronchogram” in two patients suffering from sand aspiration.2 Both of these patients exhibited particulate matter filling the bronchial tree as evidenced by radiodense material lining the central tracheobronchial tree in one case and linear radiodense opacities in the other. In reported cases of particulate aspiration following accidental burial or cave-in, similar classic sand bronchograms have been reported.3,4 Other findings on x-ray are highly variable, ranging from near normal imaging to pulmonary edema characterized by fluffy, confluent, nodular perihilar opacities.2,4 The general pattern is that of opacification of the airway involved in aspiration.
More recent reports have included CT imaging of sand aspiration, though it is not routinely obtained and reports specifically detailing CT findings are limited in number.4 In a recent retrospective examination of post-mortem CT, as opposed to conventional autopsy in the diagnosis of drowning victims, sand and sediment in the bronchial tree were visualized on nearly half of the drowning victims.5 This finding raises the possibility that sand aspiration has been historically under-recognized in drowning and near-drowning incidents.
On CT, it may be possible to appreciate sand bronchograms in the form of radiodense material filling the bronchial tree, similar to those previously described for plain chest films. These findings may be more apparent in CT imaging when relatively subtle on chest x-ray.4 Additionally, aspirated material may be visible in the trachea as radiodensities, as it was in this case’s presentation. Findings of air fluid levels in the sinuses, while nonspecific and present in a wide variety of situations, can be suggestive of either drowning or aspirated material.5 Dunagan, et al reported findings of air-fluid-sand levels in the maxillary sinuses in one near drowning patient with sand aspiration. CT is not routinely recommended in drowings, however, the true utility of CT in these instances has not been determined.3,4 In the setting of conclusive plain film radiographic findings, CT may not be necessary.
There is increasing interest in the use of post-mortem CT in the evaluation of drowning patients which may in time be expanded to use in near-drowning and other causes of sand aspiration with equivocal chest x-ray findings. Post-mortem CT may be especially valuable in determining the course of events and progression of injury leading to death.