Image
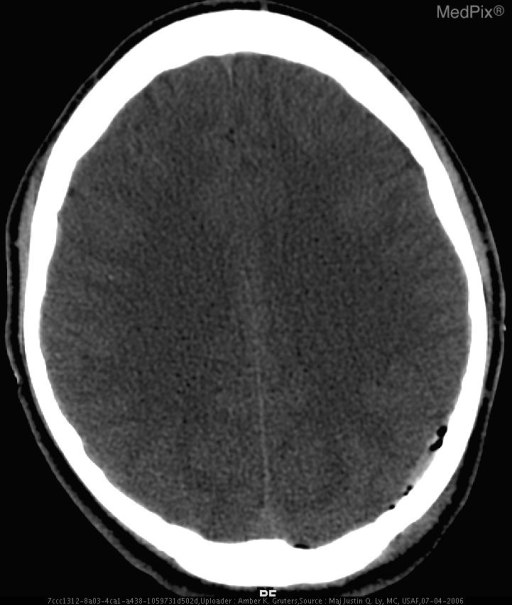
Acute Subdural Hematoma with temporal bone fracture
- Image ID
- MPX1212_synpic29914
- Case U_id
- MPX1212
- Modality
- CT · CT - noncontrast
- Plane
- Axial
- Location
- Brain and Neuro (Head)
- Age / Sex
- 18 / male
- Caption
- Axial non contrast head CT image shows a crescent-shaped extraaxial hyperdense fluid collection in the left parieto-occipital subdural space, consistent with an acute subdural hematoma. There is air in the subdural and subarachnoid space suggesting a dural breach from a fracture.
- ACR Codes
- 1.4
Clinical case
- History
- An 18-year-old Hispanic man was brought by ambulance to the Emergency Department following a high-speed motor vehicle collision in which the patient was ejected from his vehicle.
- Exam
- He was lethargic on presentation, but without evidence of any focal neurological deficits. Physical examination in the trauma bay showed swelling over his left temporal region and scattered facial abrasions.
- Findings
- Figure 1: Axial CT without contrast The noncontrast head CT revealed a small hyperdense subdural hematoma, consistent with the acute injury (Fig. 1a). There is pneumocephalus, seen as small bubbles of air within the left extraaxial parietal subdural collection as well as a single focus of air posteriorly at the left paramidline aspect of the extraaxial space shown (Fig. 1a). These findings indicate that a fracture has occurred, allowing communication of outside air or a sinus cavity with the intracranial space. Indeed a complex adjacent temporal bone fracture was detected and is best appreciated using bone windows (Fig. 1b).
- Differential Diagnosis
- Epidural hematoma Subdural hygroma Subdural empyema
- Case Diagnosis
- Acute Subdural Hematoma with temporal bone fracture
- Diagnosis By
- Radiographic findings and clinical presentation
Topic
- Category
- Trauma
- ACR Code
- 1.4
Disease discussion
The inner (or "meningeal") layer of dura contributes to the formation of the falx cerebri, tentorium, and falx cerebelli. SDHs are to be anticipated along these structures since there is a continuation of the potential subdural space along these dural reflections. Interhemispheric fissure and tentorial leaf SDHs are commonly seen in elderly trauma victims, especially if they are alcoholic. The enlarged subarachnoid spaces of these patients may contribute to an excessive mobility of the brain and greater susceptibility of the interhemispheric/tentorial veins to traumatic injury.
Acute subdural hematomas can be classified as "simple" or "complicated," depending on whether parenchymal brain injuries (contusions, intracerebral hematomas, diffuse axonal injury) are also present. Notably, intra-axial injuries are much more common with acute SDHs than with either EDHs or chronic SDHs. The majority of patients with acute SDHs, in fact, will have associated parenchymal brain injuries. Secondary forms of brain injury (anoxic/ischemic injury, trans-tentorial/subfalcine/tonsilar herniation, increased intracranial pressure) are also quite common in patients with acute SDHs.
Acute SDHs still carry a significant risk of morbidity and mortality. The overall mortality of patients with acute SDHs is greater than that for any other traumatic intracranial mass lesion (ICH, EDH, focal contusion). Despite modern therapy, the mortality is over 35% in all large series and greater than 50% in most reports. A primary factor related to clinical outcome of patients with acute SDHs is the presence or absence of associated intraaxial lesions. In one series of patients, the mortality of "simple" SDHs was 22% as compared to over 50% for those with "complicated" SDHs. A second major factor significantly related to outcome is the presence and severity of mass effect. Mass effect from a SDH may be due to a combination of factors; the hematoma itself, underlying parenchymal injury, intracerebral hematoma, and diffuse cerebral edema/swelling from a loss of vasomotor autoregulation. The mass effect can produce injury to the brain through a generalized increase in intracranial pressure, global or localized impairment of blood flow, transtentorial/tonsilar herniation resulting in ischemic/pressure necrosis of the upper brain stem. Other factors directly related to a poor outcome are; greater age of the patient, low Glasgow Coma Scores at the time of operation, bilateral lesions, rapid rate of SDH accumulation, and delayed surgical evacuation (> 4 hours) of the SDH.